




How to Best Invest in your Bones
The importance of peak bone mass
- Healthy bones are essential throughout our lives
- Bones are living tissues that continuously undergo regeneration with removal of old bone and replacement by new bone
- During times of growth (children and teenagers), more new bone is laid down than what is removed and so bones get bigger, denser and stronger
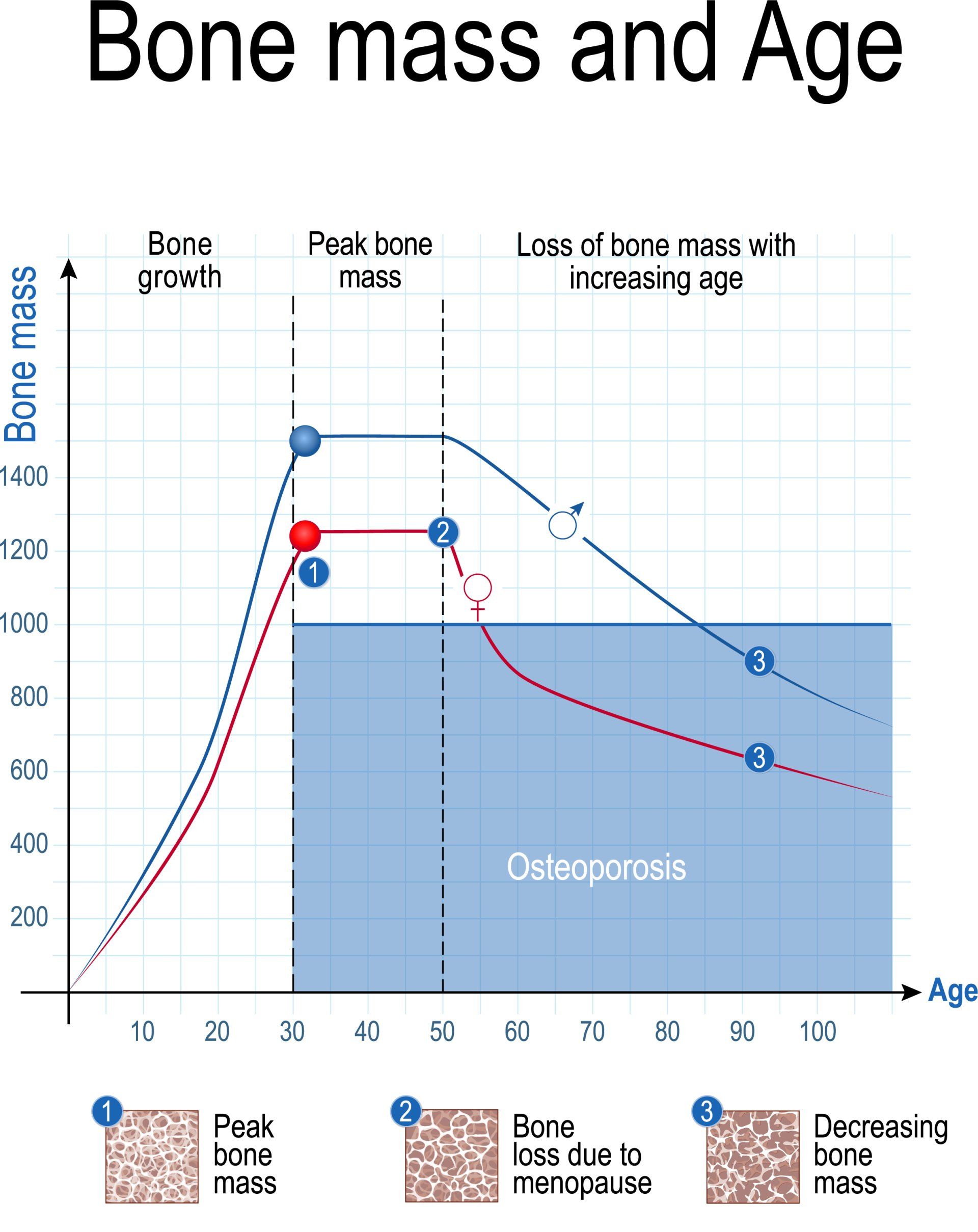
- This process continues until peak bone mass is achieved which is when the bones are at their strongest and most dense
- Peak bone mass occurs typically in late 20s and after that the balance slowly changes and bone resorption outpaces new bone formation
- Around 90% of peak bone mass is accumulated by 18 years for women and 20 years for men
- Therefore, the first 20 years of life is the best time to invest and accumulate as much bone as possible which is achieved with optimal levels of vitamin D, calcium and exercise
- Men overall achieve a larger peak bone mass than women
- Between 30 years and menopause, women (like men) have minimal change in total bone mass
- After menopause though, women experience a rapid bone loss which then slows down
- If it drops low enough it can lead to osteoporosis
- It is therefore prudent to invest as much as possible in the earlier years to maximise the peak bone mass and to continue to take measures to reduce the rate of bone loss later in life
- A 10% increase in peak bone mass can postpone development of osteoporosis by 13 years

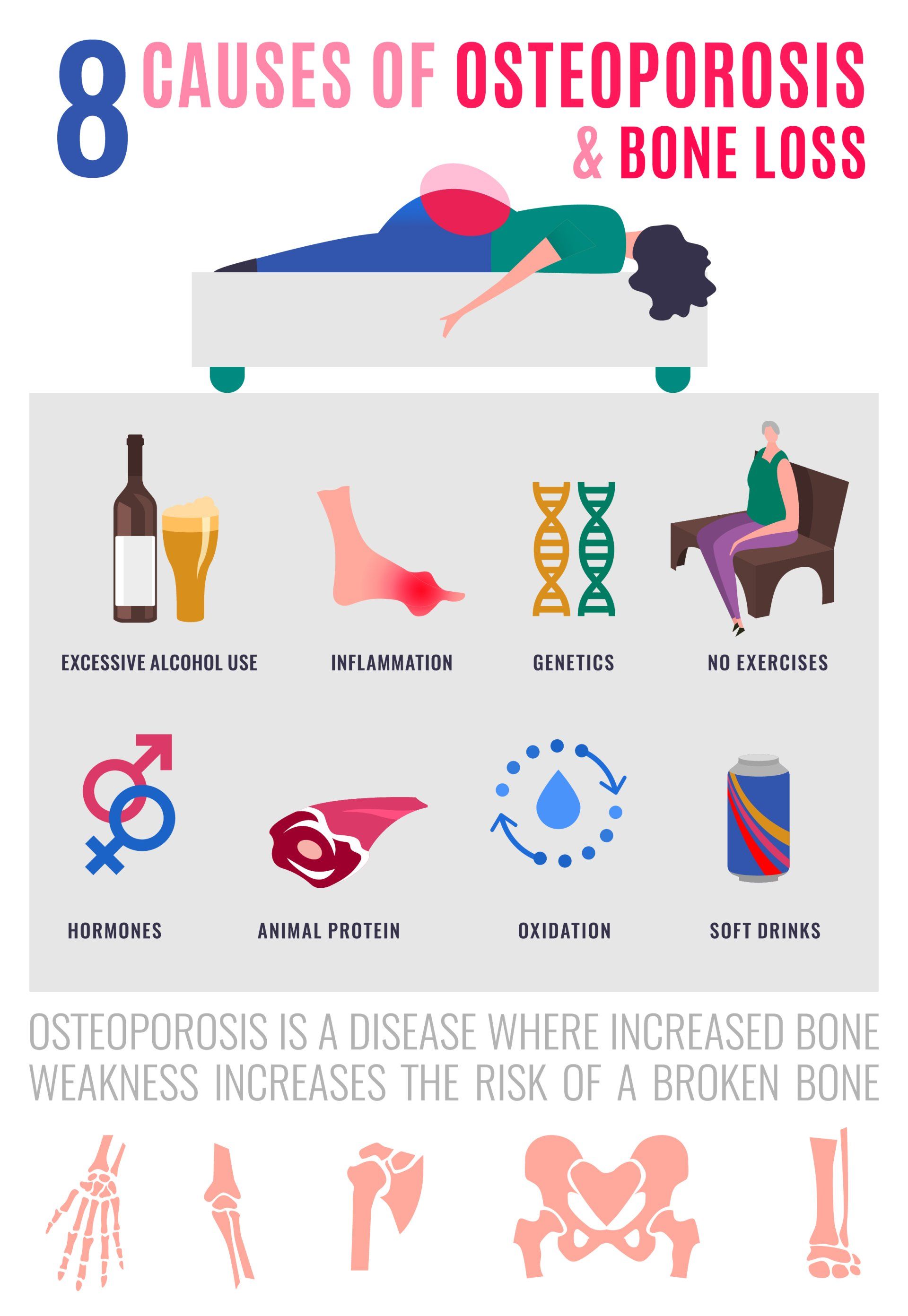
Factors that affect peak bone mass and risk of osteoporosis
- Numerous factors affect peak bone mass
- Genetic:
- These are factors you are born with and cannot change e.g. age, gender, race, body size, and family history
- Thought to have the biggest impact ~75%
- Over 60 genes have already been identified in relation to bone mineral density
- Environmental:
- These are factors that surround you throughout life e.g. exercise, diet, hormonal, medication, lifestyle, smoking, and alcohol
- Less of an impact but the only ones that can be modified ~25%
- Age:
- As one gets older the risk of osteoporosis increases and this is due to:
- Reduced protective effect of sex hormones
- Increased risk of vitamin D insufficiency
- Reduced calcium absorption
- Reduced stresses on bones from less exercise and muscle mass
- Gender:
- Males tend to have bigger peak bone mass than women
- Before puberty boys and girls have similar rates of growth in their bone masses
- After puberty, boys acquire bone at a great rate and this continues until ~30 years
- Women lose bone at a greater pace after the menopause and because they have lower peak bone mass they have less bone to lose
- Women as a result are 4 times as likely as men to develop osteoporosis
- Race:
- African American and Hispanic females manage to achieve greater peak bone mass than white and Asian females and as a result they are more protected against osteoporosis
- Body size:
- Small framed individuals (more common in women) are at greater risk as they have less bone stock in reserve to draw from as they age
- Family history:
- Positive family history of osteoporosis has been shown to greatly affect the patient’s risk of osteoporosis but also their peak bone mass
- Hormonal:
- Oestrogen has a protective effect on bones by inhibiting bone resorption:
- This is the process by which bone is broken down by bone cells called osteoclasts
- This means that the longer women are exposed to oestrogen the greater the benefit for their bones
- Women who start their menstrual cycles younger and start their menopause later have had longer exposure to oestrogen and so reach a greater peak bone mass
- Abnormal cessation of periods (amenorrhoea) such as due to extremely low body weight (anorexia) or from excessive exercise (e.g. Female Athlete Triad) or low oestrogen levels in postmenopausal women and those on certain treatments for breast cancer all increase the risk of osteoporosis
- Men with low testosterone levels (e.g. following chemotherapy for prostate cancer) have increased risk of osteoporosis:
- Testosterone stimulates cells in bone called osteoblasts to lay down new bone
- A small portion of testosterone is normally converted to oestrogen and this has been shown to be the bigger determinant of bone health in men
- Other hormones that can increase risk of osteoporosis are overactive thyroid, parathyroid and adrenal glands
- Nutrition:
- Calcium is an essential mineral required for bone mineralisation and consequently bone strength (see below)
- Calcium deficiency can have a significant impact on peak bone mass
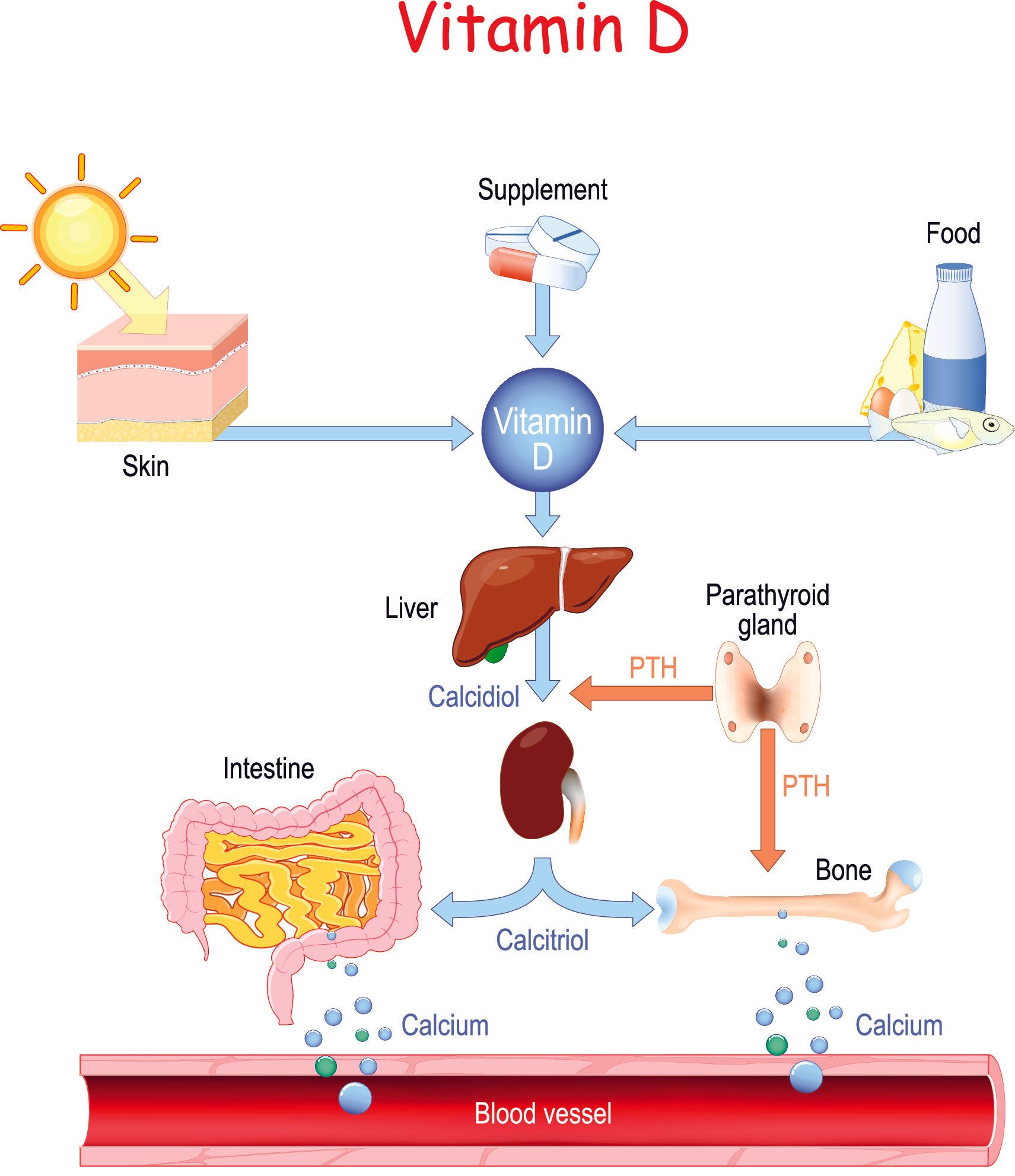
- Vitamin D deficiency is a well-known risk factor for development of osteoporosis and a key nutrient together with calcium in the initial treatment against osteoporosis
- Surgery that has removed parts of stomach or intestine can reduce the amount of nutrients (e.g. calcium) that are absorbed
- Diets low in protein have an adverse effect on bone strength
- Consumption of soft drinks with inorganic phosphate additives such as Colas increases the risk of fragility fractures
- Exercise:
- Exercise is essential for bone health throughout life
- Bones are living tissues and they get stronger when under stress
- Hence people who live a sedentary lifestyle or patients who lie in bed for periods of time and astronauts exposed to low gravity for periods of time have weakened bones
- Gentle aerobic exercise like walking is insufficient to improve bone strength
- More brisk walking and hiking are more beneficial than normal walking
- Exercises like cycling and swimming whilst being a great aerobic exercise they are considered low impact and do not make bones stronger and in fact if not combined with other strength and resistance training can weaken the bones
- Strength and resistance training:
- The heavier the weights one can lift the more beneficial for the bones
- Therefore, for bone health lifting a heavier weight less times is more beneficial than a lighter weight more times
- High impact activities such as jumping, sprinting and plyometrics are very beneficial for building bone strength because they subject the bones to multiple times the body weight over a fraction of a second that the foot is in contact with the ground
- Exercise has the added benefit of helping to improve muscle strength, balance, coordination, reaction times all of which help prevent falls and fractures:
- This is especially important for people with osteoporosis and the elderly
- A medical consultation should be considered prior to commencing exercise for those over 40 years or have health conditions such as heart problems, high blood pressure, diabetes or obesity
- In the presence of osteoporosis care should be taken when exercising in order to minimise risk of fracture:
- Avoid movements that bend or twist the spine
- Avoid high impact activities e.g. running, jumping
- Lifestyle behaviours:
- Smoking:
- Smoking is thought to inhibit the action of cells that lay down new bone called osteoblasts
- It increases the breakdown of oestrogen which is known to have a protective effect
- Reduces body weight which has adverse effect on bone density
- Induces an earlier menopause
- Reduces calcium and vitamin D absorption
- It increases production of cortisol in the body (a naturally occurring steroid)
- The impact of smoking is more drastic when it starts at a younger age and in heavy smokers
- Alcohol:
- Consumption of >4units/day is detrimental to bone strength
- Sedentary lifestyle:
- Bones become weaker as they are subjected to lower stresses
Prevention
- By maintaining a healthy lifestyle, exercise and nutrition throughout life, is the best investment in achieving as strong bones as possible early in life and therefore minimising the risk of developing osteoporosis later in life
- The genetic factors which have the greatest influence on someone’s risk of osteoporosis cannot be modified, so the focus will need to be on optimising the aforementioned modifiable risk factors
The role of calcium
- Calcium is a mineral:
- >99% is found in bones and teeth
- It adds strength to the bones and helps them withstand stresses
- A mineral is a chemical element (inorganic substance) that is an essential nutrient required by the body in order to carry out functions necessary for life
- Essential nutrient is one that is required by the body to carry out its normal functions:
- They cannot be synthesised from other ingested nutrients
- There are four groups of essential nutrients:
- Minerals
- Vitamins
- Essential fatty acids
- Essential amino acids
- Calcium is the most abundant mineral in our bodies:
- The other major minerals in the body are phosphorus, potassium, sodium and magnesium
- Since calcium is a mineral it cannot be made in the body and so it must be absorbed from food that is consumed
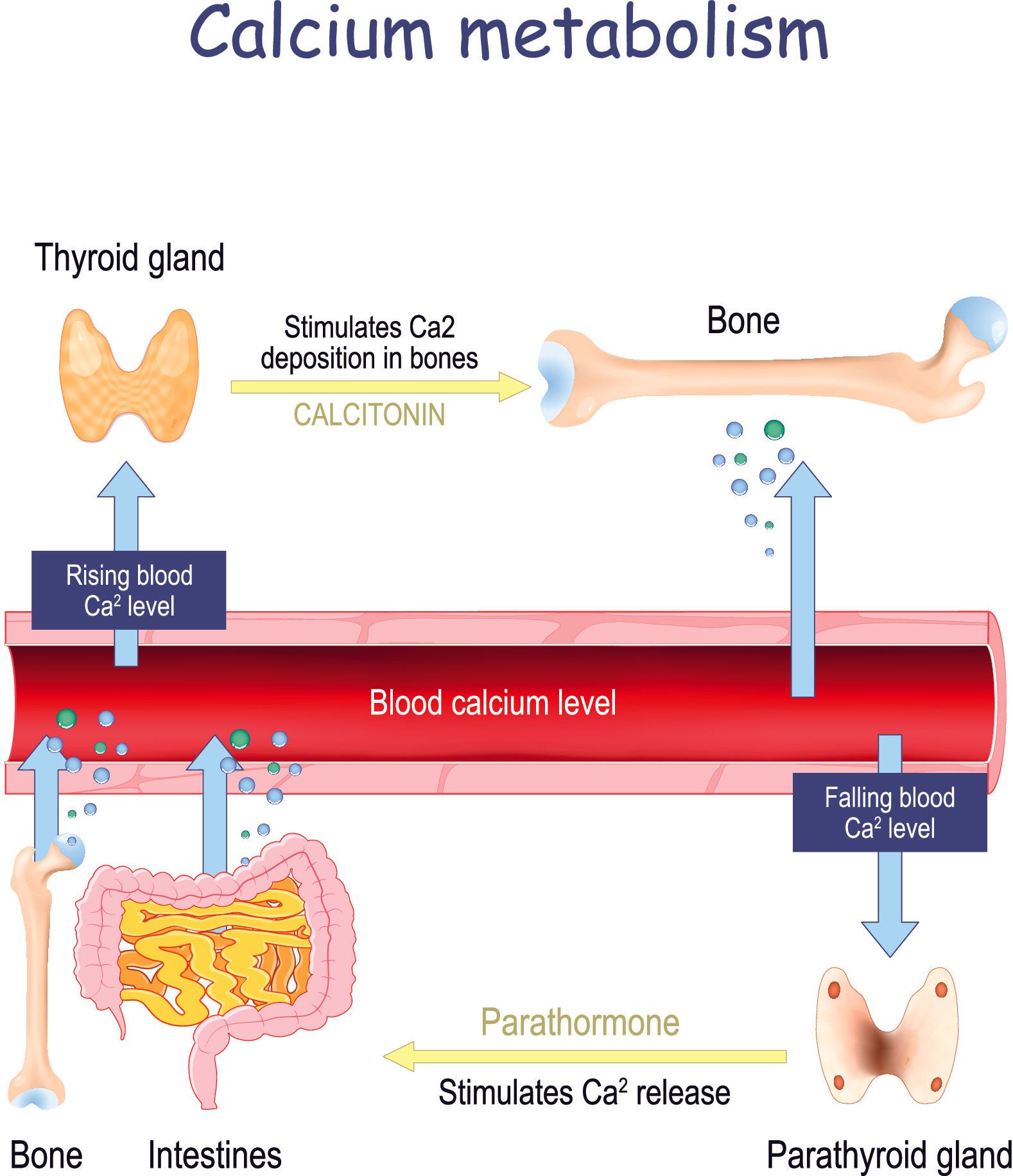
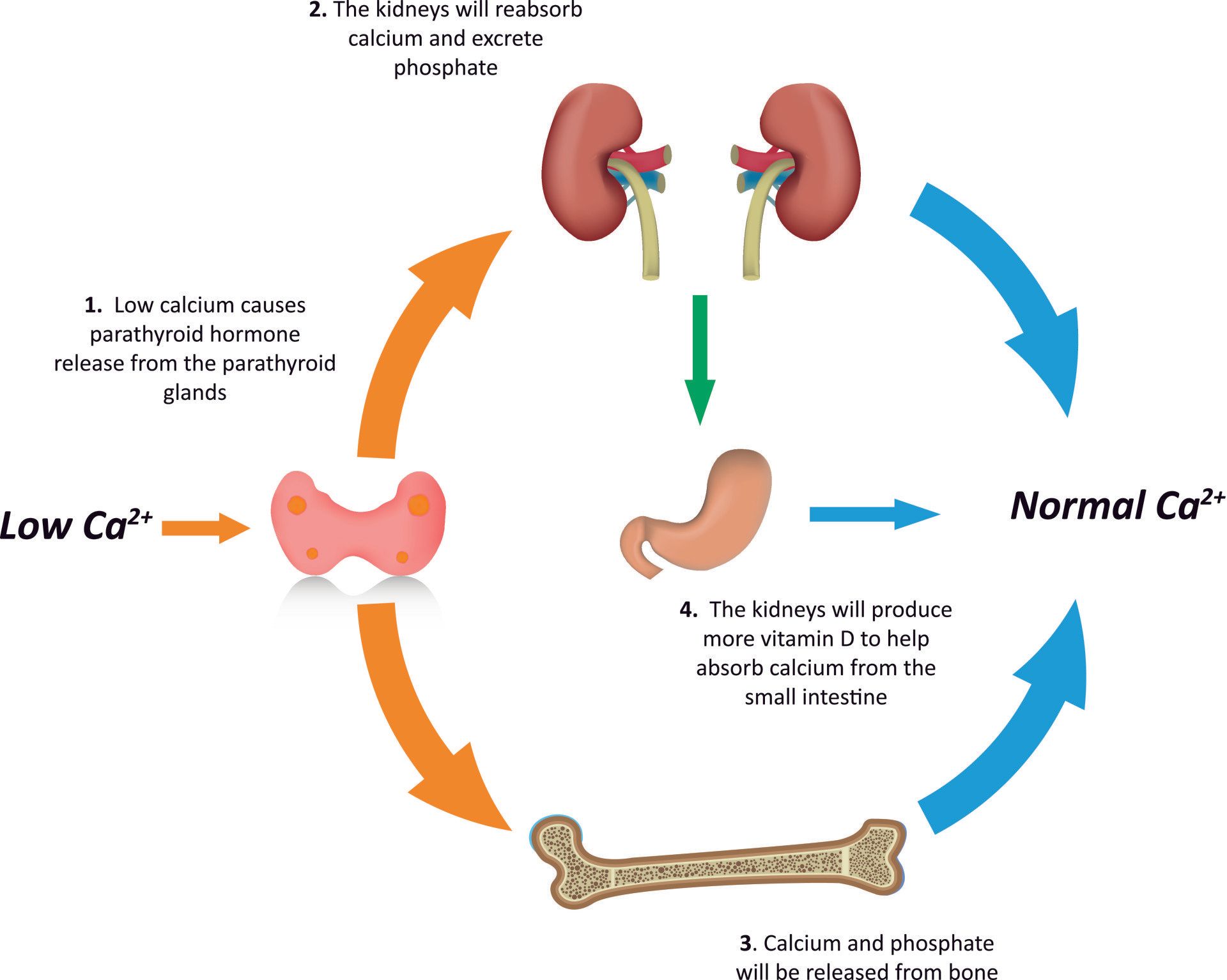
- If there is inadequate consumption of calcium, then bone is broken down as it has the largest reserves of calcium in the body (increased activity by bone cells called osteoclasts) and calcium is released into the bloodstream:
- Over time this will reduce bone mineral density, and therefore weaken the bones and lead to osteoporosis
What is the daily recommended intake of Calcium?
- The recommended daily intake varies for men and women and also varies with age:
Recommended Daily Allowance in milligrams (mg)
| Group | Age | Recommended Daily Calcium Intake (mg) |
|---|---|---|
| Men and Women | 9-18 years | 1300 mg |
| Men and Women | 19-50years | 1000 mg |
| Men | 51-70 years | 1000 mg |
| Women | 51-70 years | 1200 mg |
| Men and Women | >70 years | 1200 mg |
| Pregnant or nursing women | 14-18 years | 1300 mg |
| Pregnant of nursing women | 19-50 years | 1000 mg |

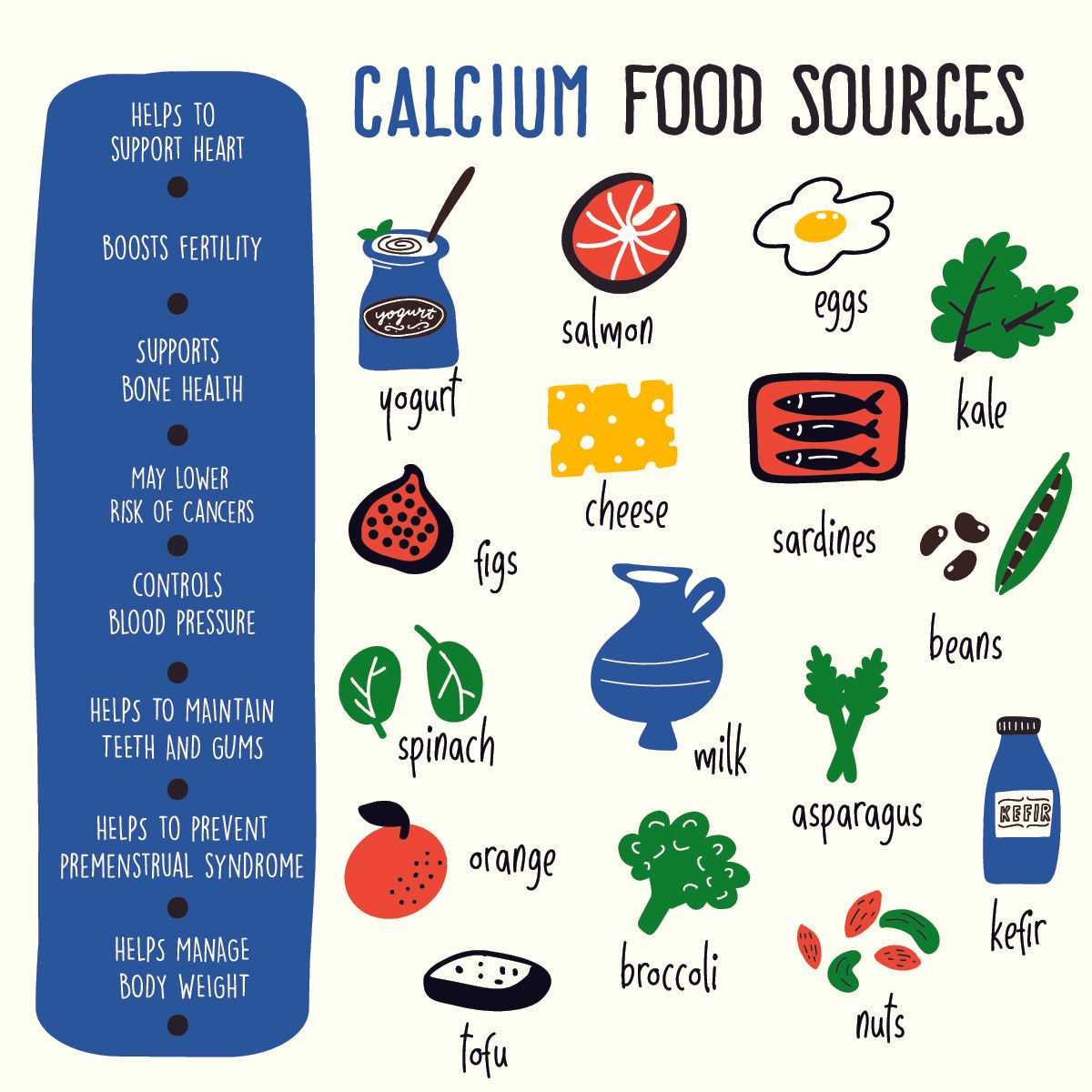
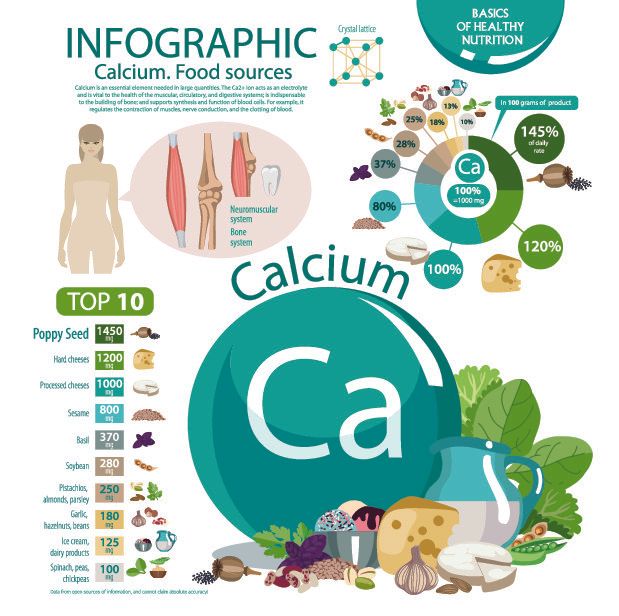
Which foods have high calcium?
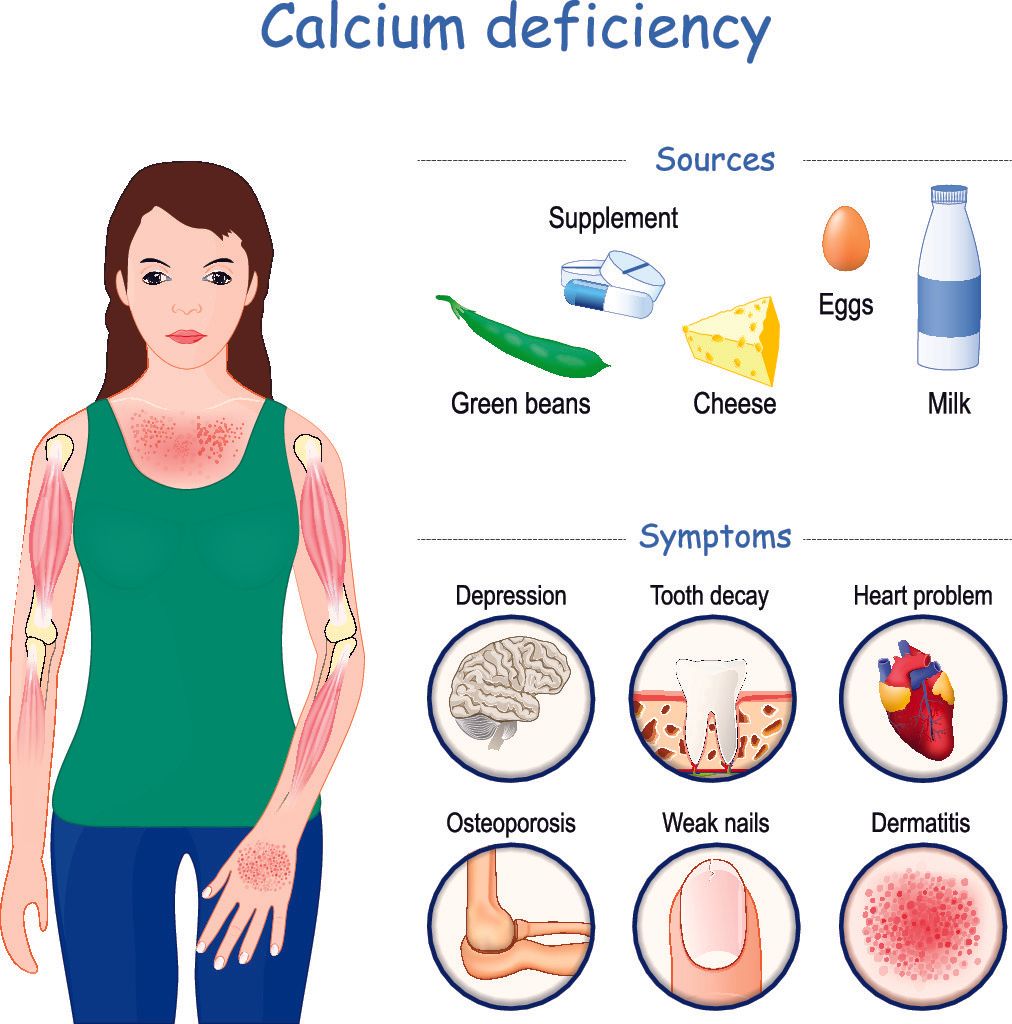
- Dairy products are the biggest sources of calcium:
- Milk, yoghurt, cheese
- Other sources are:
- Broccoli, kale, green leafy vegetables
- Salmon, sardines, other soft bone fish
- Tofu
- Bread, pasta, grains
- Cereals fortifies with calcium
What are the symptoms of low calcium?
- Low vitamin D causes reduced calcium absorption and this in turn causes:
- Osteoporosis and osteopaenia
- Fatigue:
- Low energy and feeling tired
- Dizziness
- Sleepiness
- Muscle problems:
- Cramps
- Muscle ache and spasms
- Neurological:
- Paraesthesia (pins and needles) or numbness to hands, feet and around mouth
- Confusion
- Memory loss
- Hallucinations
- Skin problems:
- Dry and itchy skin
- Eczema:
- Inflammation of the skin leading to itchiness and skin to be cracked and rough
- Psoriasis:
- A chronic autoimmune disorder where skin cells multiply 10 time faster than normal
- Leads to scaling of the skin typically over knees, elbows and scalp
- Can also lead to arthritis of joints such as the knee
- Alopecia:
- Autoimmune disorder leading to hair loss
- Weak and brittle nails
- Painful Premenstrual Syndrome:
- Daily supplementation with 500mg/day can significantly reduce premenstrual depression, fatigue, oedema and pain in women with Premenstrual Syndrome
- Dental Problems:
- Weak roots, brittle teeth, tooth decay
- In infants this can lead to delay in tooth formation
Further helpful information can be found here on:

Introduction De Quervain’s tenosynovitis (also called De Quervain’s tendinosis) is a painful condition of two tendons at the level of the wrist on the side of the thumb It’s a repetitive strain injury due to overuse of two tendons used to move the thumb away from the other fingers

Introduction Cubital Tunnel Syndrome occurs when the ulnar nerve is compressed within a tunnel on the inner (medial) side of the elbow just behind the bony prominence of the inner aspect of the elbow called the medial epicondyle Cubital Tunnel Syndrome is the second most common cause of peripheral nerve compression: The most common one being carpal tunnel syndrome (compression of the median nerve at the wrist) The ulnar nerve is one of the three main nerves of the upper limb: The other two nerves of the upper limb are the median nerve and the radial nerve The ulnar nerve travels from the neck past the elbow and wrist and into the hand: Along the way it travels past some narrow areas where it can be constricted and cause symptoms for the patient The most common site of ulnar nerve compression is in the cubital tunnel at the elbow The second most common site is in Guyon’s canal in the hand When someone accidentally hits the inner side of the elbow (often termed hitting the funny bone) they get a sharp tingling sensation on the inner side of the elbow and forearm: This occurs because the ulnar nerve was hit at the site of the cubital tunnel where the nerve is close to the skin surface and therefore easily injured from outside forces
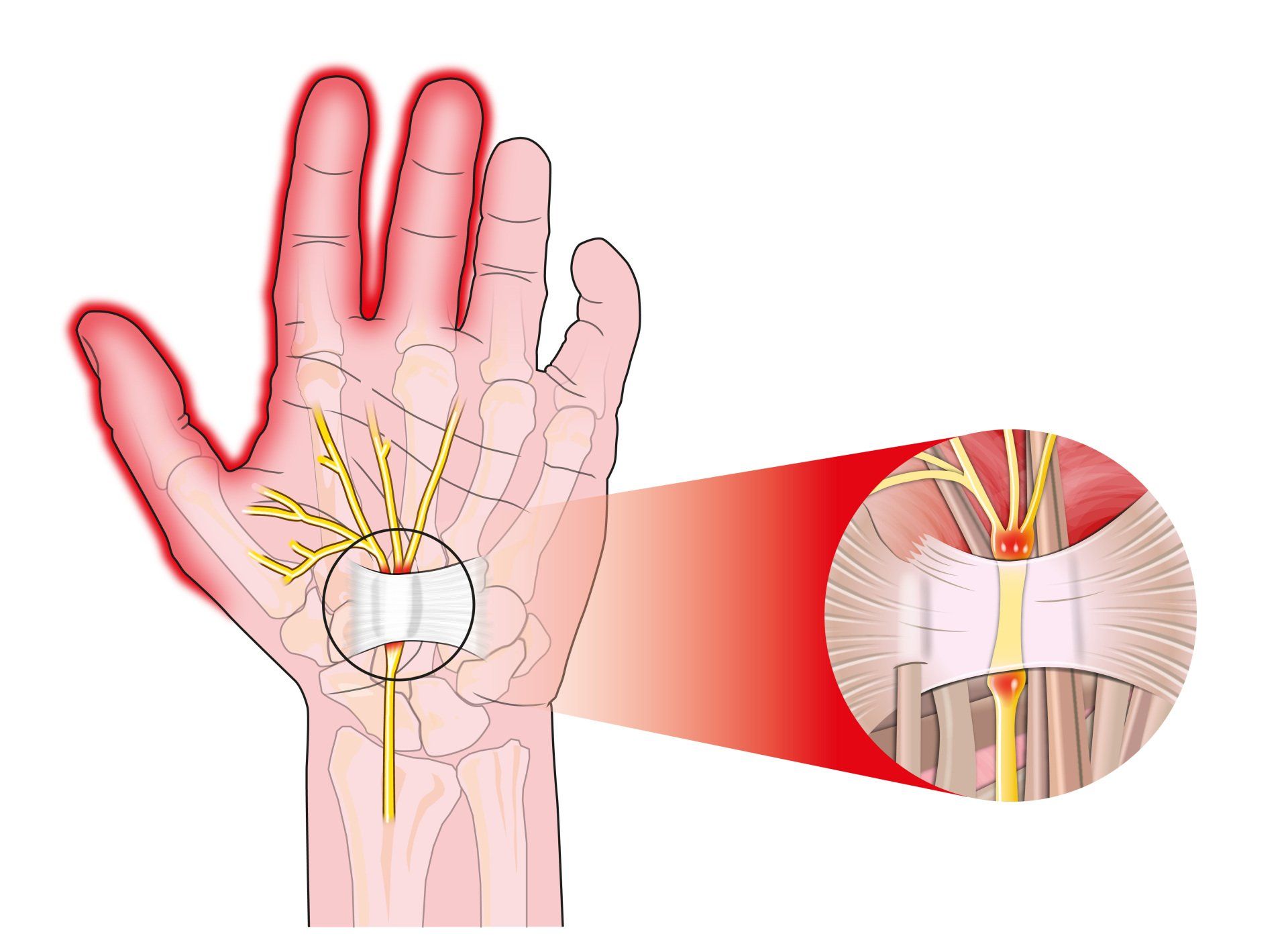
Introduction Carpal tunnel syndrome is a common condition that causes numbness, tingling and weakness in the hand specifically affecting the thumb, index and middle fingers: The little and ring fingers are not affected as they are supplied by another nerve called the ulnar nerve It is the commonest cause of peripheral nerve entrapment It is caused by compression of the median nerve as it passes from the forearm into the hand through a passage called carpal (i.e. wrist) tunnel The median nerve is one of three main nerves that supply the upper limb: The other two nerves are the ulnar nerve and the radial nerve
Introduction Tennis elbow (also known as lateral epicondylitis) is an overuse injury of the forearm tendons that originate over the lateral epicondyle of the humerus (bony prominence on the outside of the elbow) and act to bring the wrist backward away from the palm Whilst tennis players are particular prone to this condition it does not occur exclusively to them

Introduction This term is also known as repetitive motion or stress injury and occurs as a result of carrying out the same motion repeatedly over time causing injury to muscles and tendons It is associated with repetitive tasks, sustained or awkward position, forceful exertion, vibration or compressive forces It can affect almost any joint in the body Most commonly affected areas are hands, wrists, shoulders and neck It is thought to affect 5-10% of the general population but can be as high as 20-40% in specific working populations

The most common injuries in sailing, are in the waist (45%), knees (30%) and shoulders (20%). Causes of sailing injuries, windsurfing injuries, sprain or ruptured knee ligament. Injury prevention, protective clothing to avoid injuries in sailing.

Injuries such as concussion, anterior cruciate ligament injury, anterior gonalgia, fatigue fracture, tibial periostitis, ankle sprain, rotator cuff injury should be avoided for women to exercise.

Women have a 50% higher risk of developing pathologies when running and exercising. Prevention of Sport Injuries.

It is composed of three components: Low energy availability with or without eating disorder - Menstrual disorders - Decreased bone mineral density (BMD) - Treatment

What is the function of vitamin D - The benefits of vitamin D, what amount of vitamin D should I take, which foods are high in vitamin D, risks of vitamin D deficiency, the role of the sun, osteoporosis, causes, symptoms.