




Tennis Elbow
Introduction
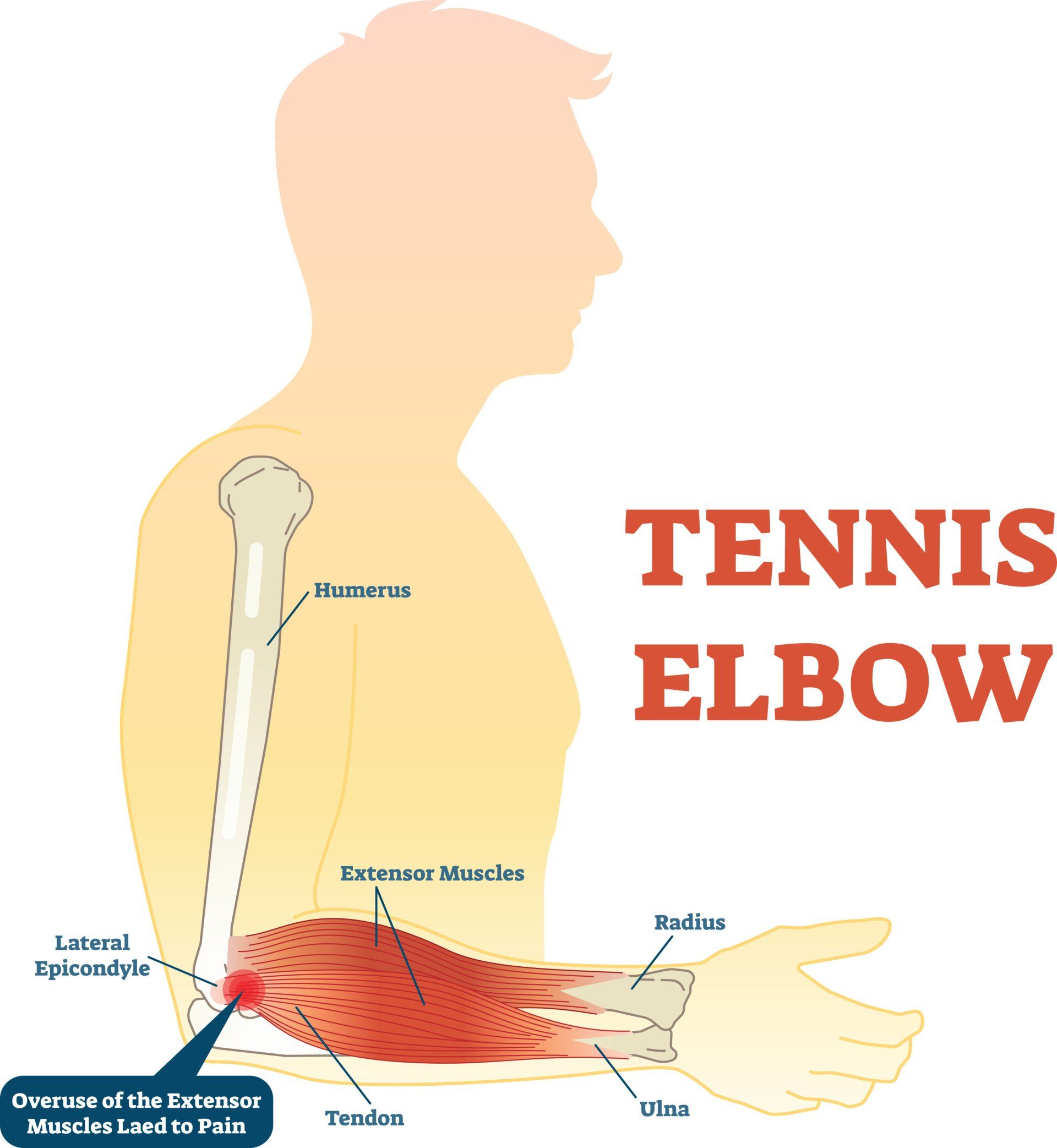
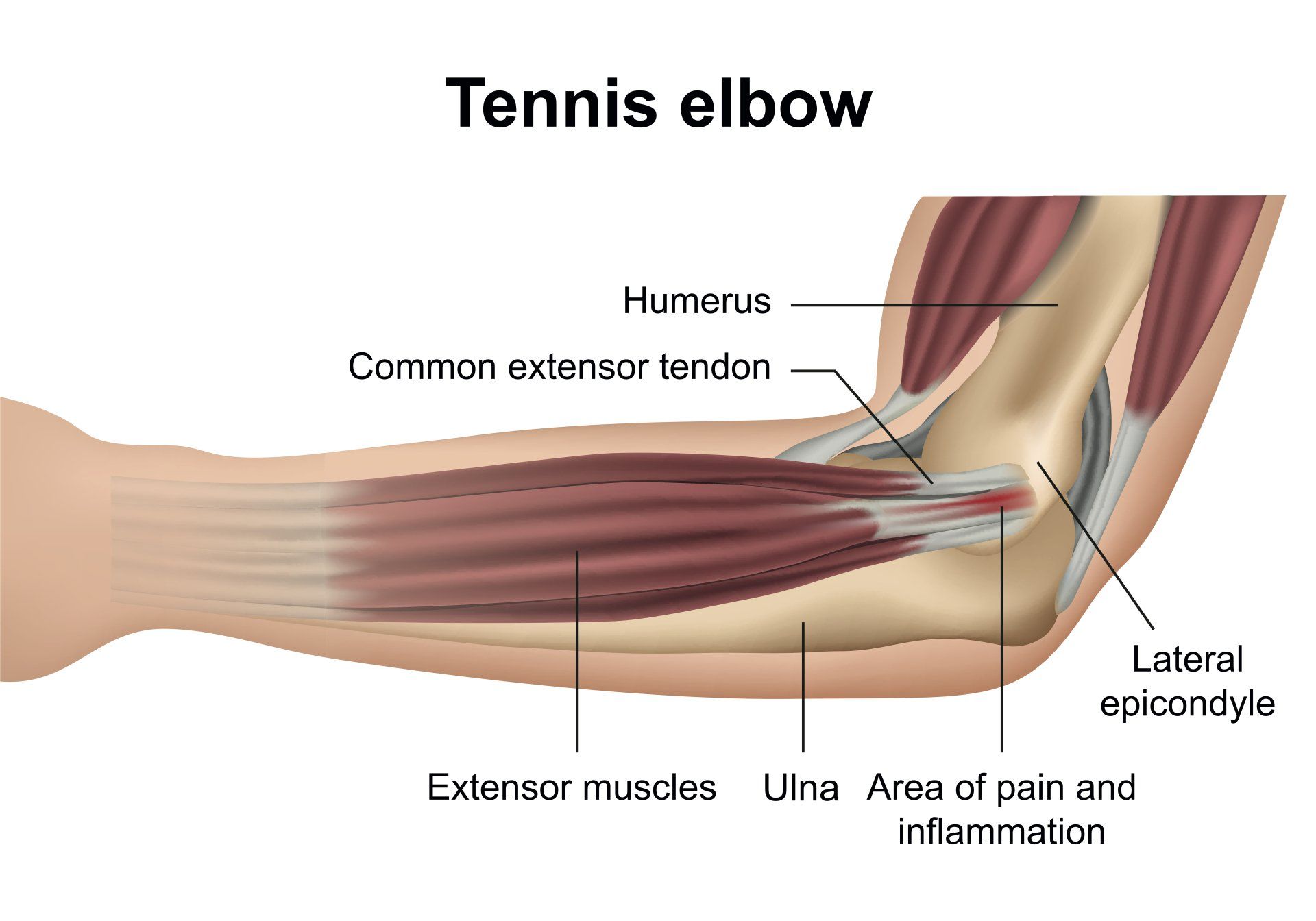
- Tennis elbow (also known as lateral epicondylitis) is an overuse injury of the forearm tendons that originate over the lateral epicondyle of the humerus (bony prominence on the outside of the elbow) and act to bring the wrist backward away from the palm
- Whilst tennis players are particular prone to this condition it does not occur exclusively to them
What causes tennis elbow?
- The forearm muscles that act to extend the wrist (lift up away from the palm) and fingers originate from the bony prominence on the outer aspect of the elbow called lateral epicondyle
- Muscles attach to a bone via a strong fibrous tissue called a tendon
- Tennis elbow arises due to injury of a specific extensor forearm muscle called extensor carpi radialis brevis (ECRB)
- ECRB is particularly active when having to extend the wrist and fingers with the elbow straight which is the most provocative position to get tennis elbow
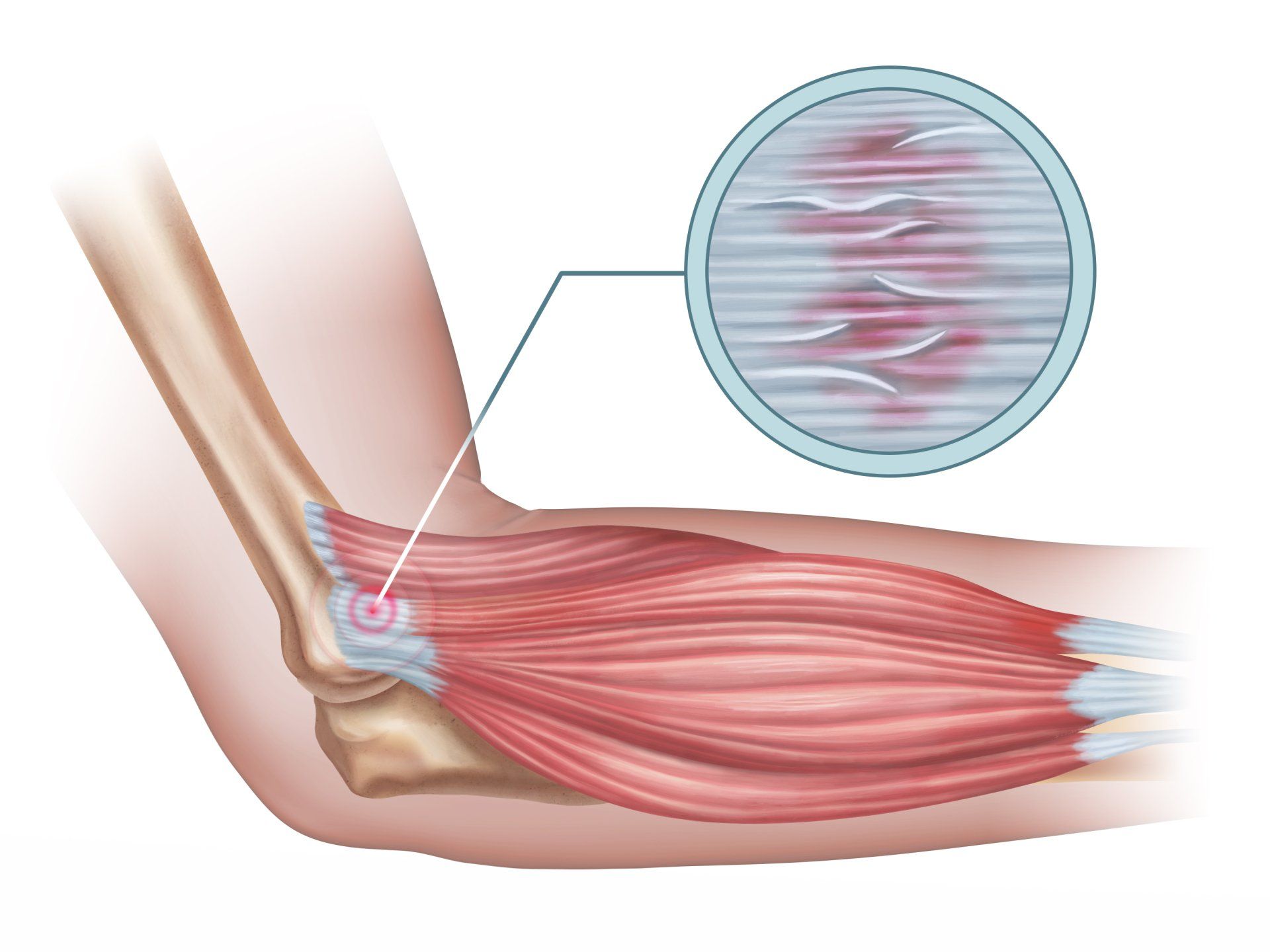
- Tennis elbow is a type of repetitive strain injury and repeated extension of the wrist causes tiny tears of the ECRB tendon weakening it and altering its structure
- Generally it is due to:
- Overuse of the wrist extensor muscles such as excessive gripping, wringing of clothes, painting, hammering, typing
- Intensifying forearm muscle activity rapidly that body is not accustomed
- Weak forearm muscles
- Poor technique such as how a backhand tennis shot is executed

Who is at risk of getting tennis elbow?
- Tennis elbow affects 1-3% of the population
- ~50% of tennis players will get suffer from tennis elbow during their careers
- <5% of cases are related to playing tennis
- Most commonly occurs between 30 and 50 years
- Males and females are equally affected
- Those who play racket sports especially tennis are at risk
- Occupations that require repetitive forearm movements are at risk such as butchers, carpenters, plumbers, musicians, painters, those who frequently use a computer or a screwdriver and hammer
Symptoms
- Presents with pain, burning or an ache on the outside of the elbow and upper forearm which is made worse by extending the wrist
- Sometimes the pain can go lower down the outer forearm
- Weak grip
- Pain when:
- Shaking hands
- Squeezing an object
- Lifting something
- Using tools such as a screwdriver or hammer
- Opening a jar
- Turning a door handle
- Gardening
Diagnosis
- History and examination are often enough to make a diagnosis
- A simple test to confirm tennis elbow is asking the patient to go behind a chair, grip the top of it with palms facing downwards and with straight elbows to lift it up:
- If this causes pain then it is positive for tennis elbow
Is Tennis elbow a tendonitis or tendinopathy
- Numerous studies have shown that there is lack of acute inflammation in tennis elbow and therefore it is not a tendinitis but a tendinopathy
- Tendinopathy is the degeneration of the normal collagen makeup of a tendon and not an inflammatory reaction like tendonitis
- Tendinopathy is caused by numerous microtears of the tendon altering its structure
- Healthy normal tendon is composed primarily of type I collagen
- Collagen is the most abundant protein of the human body:
- Collagen is found in high proportions in connective tissues, bone and skin
- It provides strength to the tissue
- In tendinopathy as a result of the body trying to heal the microtears, there is a greater proportion of the weaker type III collagen

Treatment
- Conservative treatment is very successful (~90%) if followed correctly
- Rest:
- Resting by avoiding exertional painful activities for several weeks
- Brace:
- Tennis elbow brace can be helpful
- Ice:
- In the acute phase, ice can help relieve pain
- Anti-inflammatory medication may be effective for pain relief:
- Aspirin, ibuprofen, diclofenac
- Use sparingly due to side effects when taken long term
- Steroid injection:
- Steroid injections are currently not recommended
- Research shows that even though pain may reduce after 3-6 weeks it comes back to levels worse when compared by physiotherapy alone and healing is also delayed
- Physiotherapy:
- Exercises to help strengthen the extensor forearm muscles and promote healing of the damaged tendon
- The most effective way to combat tennis elbow is through physiotherapy exercises in particular the research proven Tyler twist (described below)
- Grip strength:
- Squeeze a rolled up towel or tennis ball for 10 seconds and release for 5 seconds
- Repeat 10 times or as many times as you can and repeat on the other arm
- Supination strength:
- Whilst sitting rest your forearm on your knee so that your shoulder and elbow are lying still
- Hold a weight from one end of it e.g. a 1.5L bottle of water end on (the amount of water can be changed pending the strength and symptoms of the patient)
- Turn your palm upwards rapidly whilst holding the weight end on
- Let the weight turn your hand facing downwards slowly
- Repeat 10 times on each side
- Wrist extension:
- Whilst sitting rest your forearm on your knee so that your shoulder and elbow are lying still
- Hold a weight with your palm facing downwards
- Whilst your palm is facing down extend your wrist by bringing your wrist upwards towards your body
- Bring the weight up fast and lower it down slowly
- Repeat 10 times on each side
- Wrist flexion:
- Whilst sitting rest your forearm on your knee so that your shoulder and elbow are lying still
- Hold a weight with your palm facing upwards towards the ceiling
- Whilst your palm is facing up flex your wrist by bringing your wrist upwards towards your body
- Bring the weight up fast and lower it down slowly
- Repeat 10 times on each side
- Towel twist:
- Hold a rolled-up towel in both hands out in front of you
- Twist both wrists in opposite directions (one wrist extends whilst the other flexes) as if you are wringing out water
- Repeat 10 times in each direction
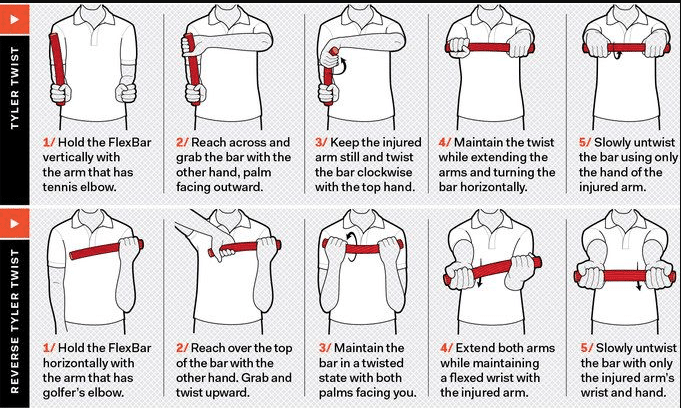
- Tyler twist:
- To do this you will need a flexible bar that you can rotate and carry out the following movements in the sequence stated
- Hold the flexible bar vertically on the painful side with the wrist in maximum extension
- Whilst keeping the flexible bar vertically, reach across and grab the opposite end of the bar with the other hand, palm facing outward
- Continue gripping the bar firmly with the wrist on the injured side in position of maximum extension and twist the bar clockwise by flexing the uninjured wrist
- Maintain the twist whilst extending both arms out in front of you and holding the bar horizontally at the level of the shoulders with the involved wrist in full extension and the uninvolved wrist in full flexion
- Using the injured arm slowly untwist the flexible bar by flexing the extended injured wrist
- Do 3 sets of 15 repetitions a day
- Surgery:
- Considered following failure of conservative treatment in 6-12 months
- Has good results long term
Further helpful information can be found here on:

Introduction De Quervain’s tenosynovitis (also called De Quervain’s tendinosis) is a painful condition of two tendons at the level of the wrist on the side of the thumb It’s a repetitive strain injury due to overuse of two tendons used to move the thumb away from the other fingers

Introduction Cubital Tunnel Syndrome occurs when the ulnar nerve is compressed within a tunnel on the inner (medial) side of the elbow just behind the bony prominence of the inner aspect of the elbow called the medial epicondyle Cubital Tunnel Syndrome is the second most common cause of peripheral nerve compression: The most common one being carpal tunnel syndrome (compression of the median nerve at the wrist) The ulnar nerve is one of the three main nerves of the upper limb: The other two nerves of the upper limb are the median nerve and the radial nerve The ulnar nerve travels from the neck past the elbow and wrist and into the hand: Along the way it travels past some narrow areas where it can be constricted and cause symptoms for the patient The most common site of ulnar nerve compression is in the cubital tunnel at the elbow The second most common site is in Guyon’s canal in the hand When someone accidentally hits the inner side of the elbow (often termed hitting the funny bone) they get a sharp tingling sensation on the inner side of the elbow and forearm: This occurs because the ulnar nerve was hit at the site of the cubital tunnel where the nerve is close to the skin surface and therefore easily injured from outside forces
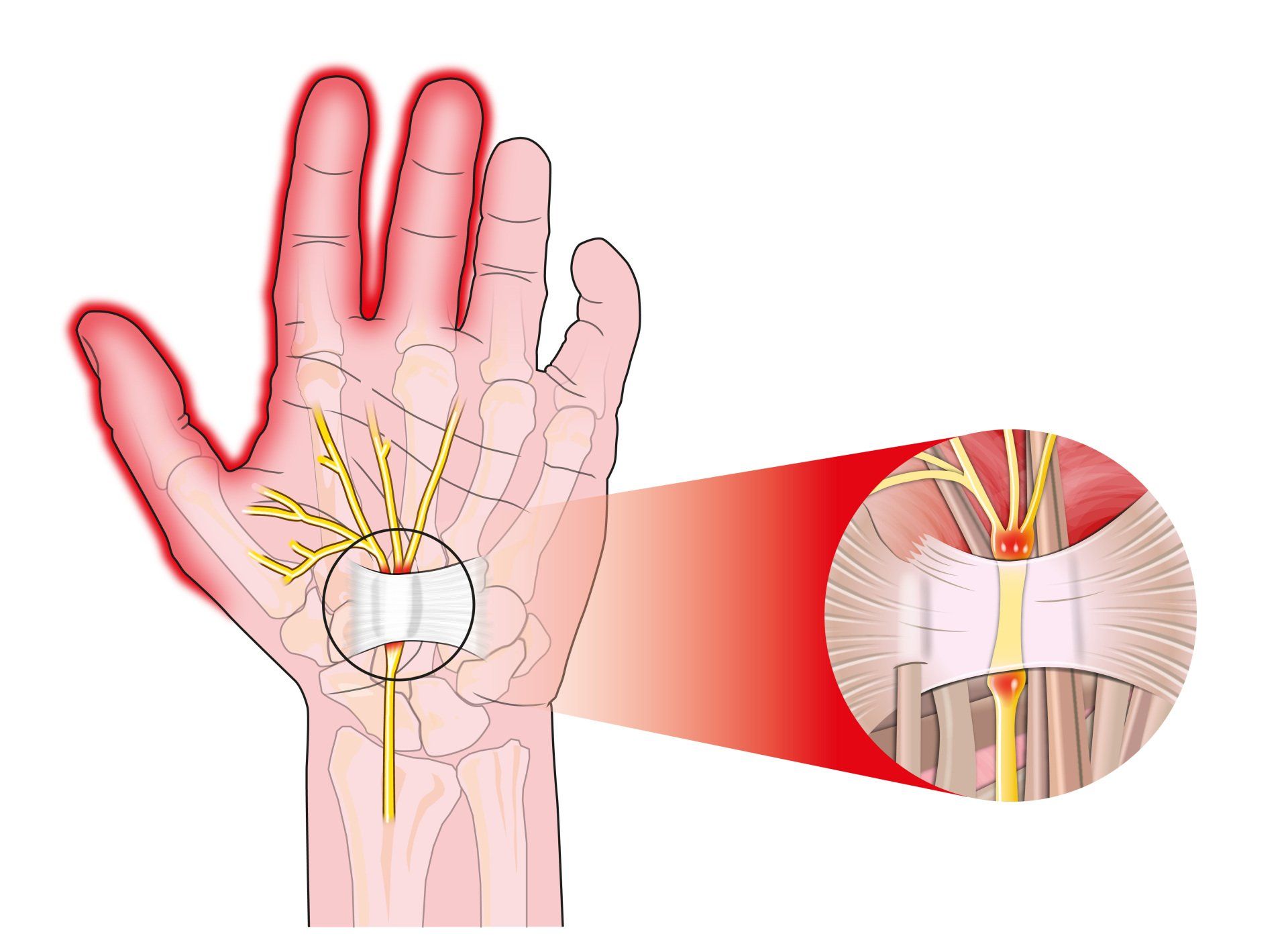
Introduction Carpal tunnel syndrome is a common condition that causes numbness, tingling and weakness in the hand specifically affecting the thumb, index and middle fingers: The little and ring fingers are not affected as they are supplied by another nerve called the ulnar nerve It is the commonest cause of peripheral nerve entrapment It is caused by compression of the median nerve as it passes from the forearm into the hand through a passage called carpal (i.e. wrist) tunnel The median nerve is one of three main nerves that supply the upper limb: The other two nerves are the ulnar nerve and the radial nerve

Introduction This term is also known as repetitive motion or stress injury and occurs as a result of carrying out the same motion repeatedly over time causing injury to muscles and tendons It is associated with repetitive tasks, sustained or awkward position, forceful exertion, vibration or compressive forces It can affect almost any joint in the body Most commonly affected areas are hands, wrists, shoulders and neck It is thought to affect 5-10% of the general population but can be as high as 20-40% in specific working populations

The most common injuries in sailing, are in the waist (45%), knees (30%) and shoulders (20%). Causes of sailing injuries, windsurfing injuries, sprain or ruptured knee ligament. Injury prevention, protective clothing to avoid injuries in sailing.

Injuries such as concussion, anterior cruciate ligament injury, anterior gonalgia, fatigue fracture, tibial periostitis, ankle sprain, rotator cuff injury should be avoided for women to exercise.

Women have a 50% higher risk of developing pathologies when running and exercising. Prevention of Sport Injuries.

It is composed of three components: Low energy availability with or without eating disorder - Menstrual disorders - Decreased bone mineral density (BMD) - Treatment

What is the function of vitamin D - The benefits of vitamin D, what amount of vitamin D should I take, which foods are high in vitamin D, risks of vitamin D deficiency, the role of the sun, osteoporosis, causes, symptoms.
Read all about osteoporosis, what causes it, frequency in women and men, fracture prevention, diagnosis and treatment.