




Anterior Cruciate Ligament (ACL) Injury
What is the burden of ACL injuries?
- 350,000 ACL reconstructions carried out annually in USA
- Cost of treatment of ACL reconstructions in USA is estimated to be around $2 billion
- If there is additional meniscal or cartilage injury there is increased risk of developing osteoarthritis
- 20% will suffer re-injury within 2 years
- Individuals at greatest risk of reinjury are men aged 20-24 years and women 15-19 years
- Revision ACL reconstructions are rising more rapidly than primary ACL reconstructions
- There is an increasing focus on ACL Injury Prevention Programmes which can reduce by half the risk of torn ACL
Mechanism of ACL injury
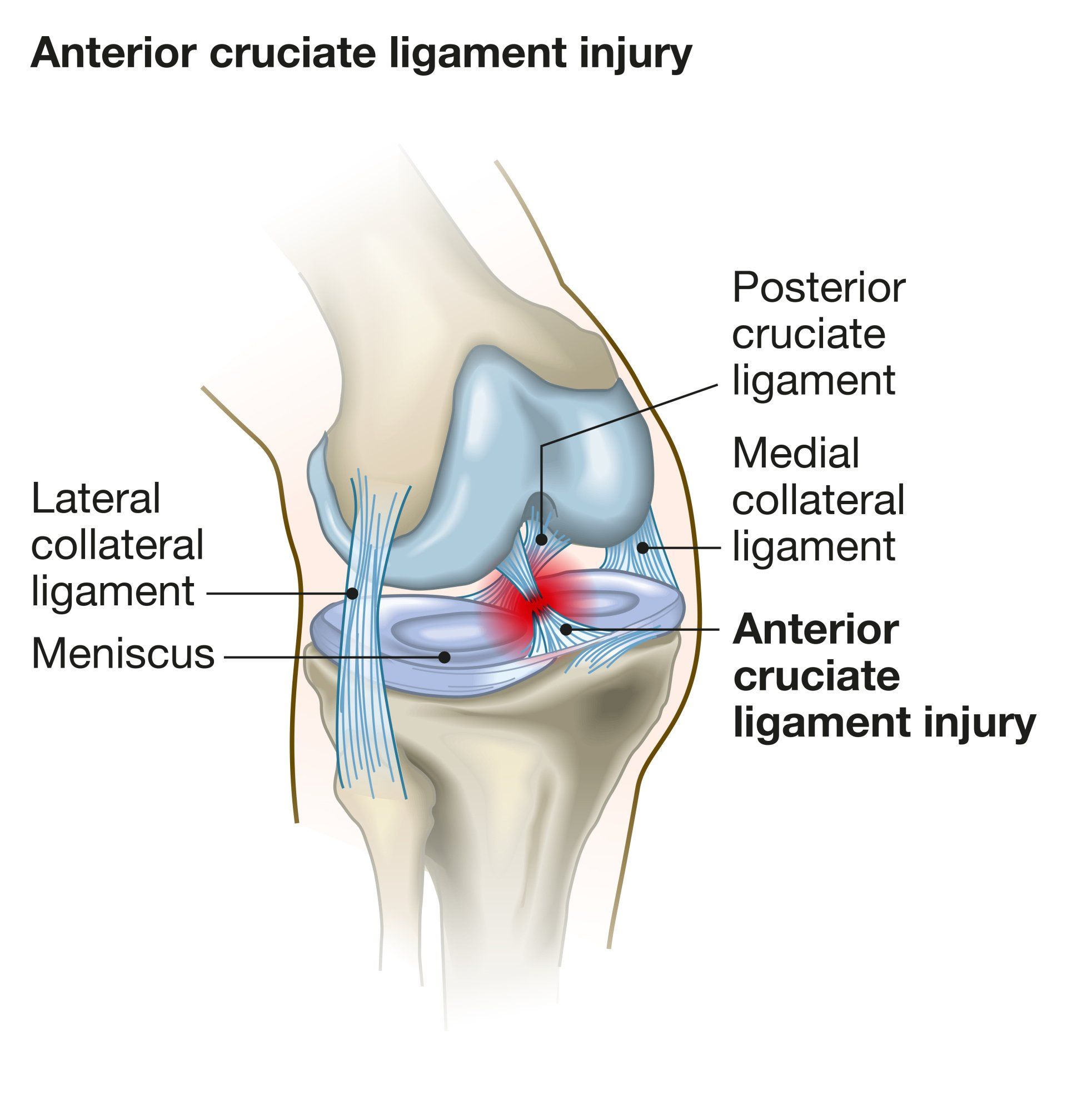
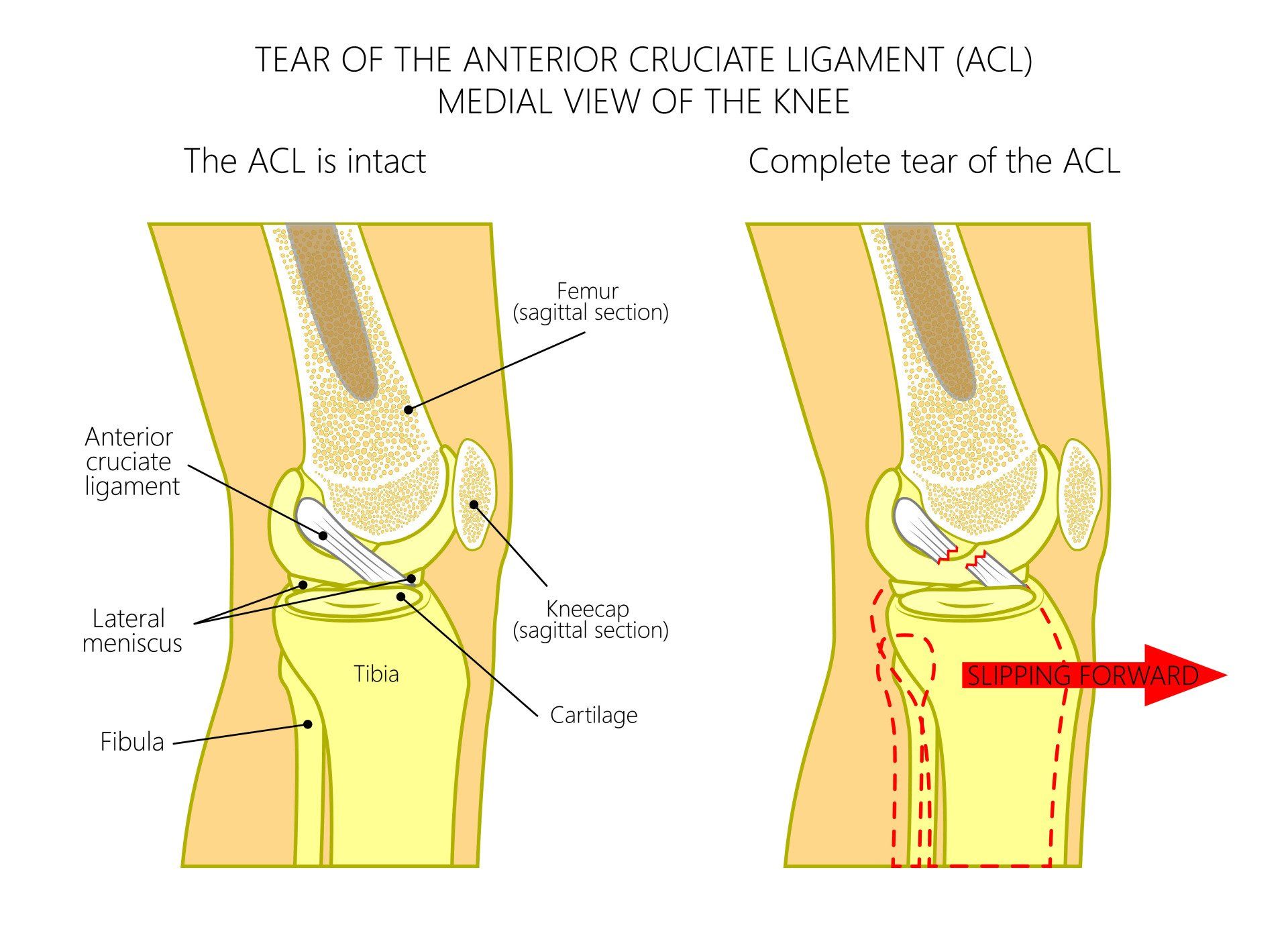
- ACL is one of the four major ligaments in the knee and it helps prevent the tibia going too far forwards in relation to the femur and provides rotational stability
- More information on ACL anatomy available here
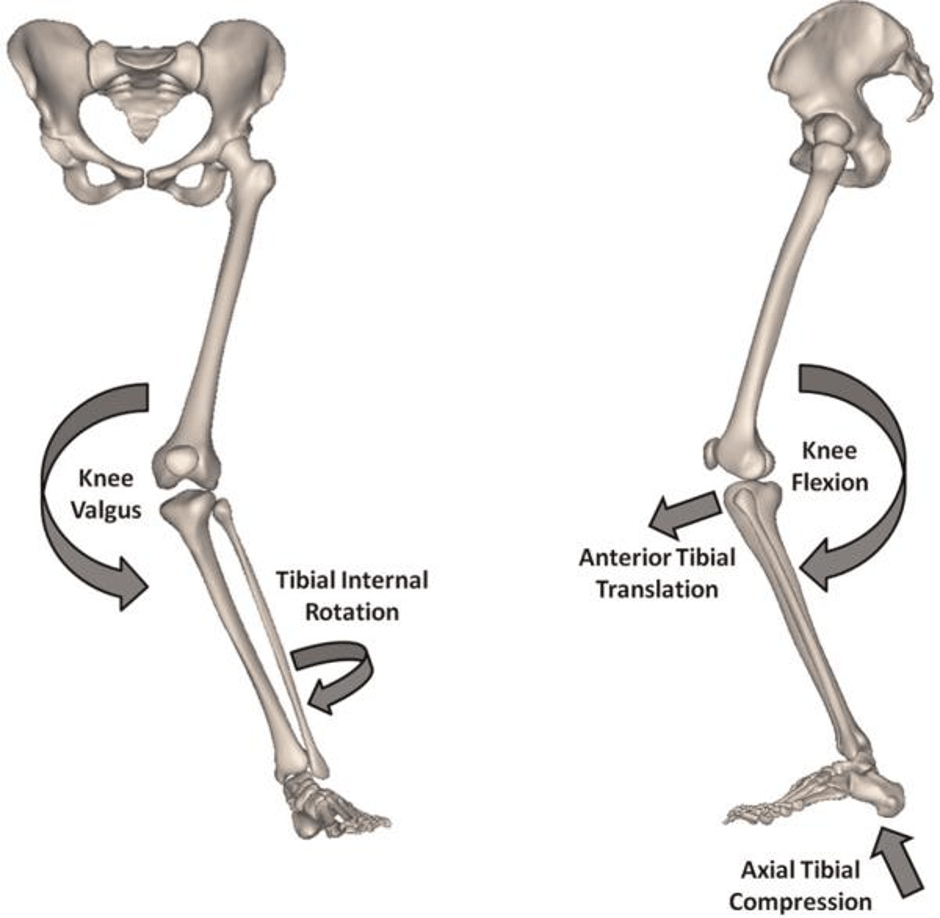
- Occurs most commonly due to a non-contact injury whilst rapidly changing direction, pivoting or landing after a jump
- The loaded slightly flexed knee (10-30 degrees of flexion) is placed in a valgus stress with the foot planted to the ground and the tibia internally rotates in relation to the femur
- Valgus stress is when the knee goes in towards the midline in relation to the ankle
- 70% of ACL injuries are due to non-contact (i.e. due to a wrong movement rather than a collision)
- Only 30% of ACL injuries are due to contact
- Rapid change in direction and speed (particularly deceleration) pose an increased risk
- ACL injury has an incidence of about 1 in 3000 in general population and 1 in 1750 in people aged 16-45 years
Who is at risk of an ACL injury?
- ACL injury is most common in sports involving pivoting:
- Football
- Basketball
- Netball (highest risk)
- Handball
- Volleyball
- Down-hill skiing
- Gymnastics
- Below are the age groups and the frequency of ACL injuries as a percentage of the total:
- < 16 y (12.5%)
- 17-25 y (32.5%)
- 26-35 y (23%)
- 36-45 y (20%)
- 46-55 y (9.5%)
- >55 y (1.5%)
- As can be seen the age group which is most commonly affected by ACL injury are 17-25 years followed by 26-35 years
How common are ACL injuries?
- ACL injuries are among the more common injuries sustained in sports
- It is thought to affect 1 in 3500 people every year
- However this could be underestimated as not all injuries are reported
How common are ACL injuries in children?
- ACL injuries are increasingly common in children due to increased competition of youth sports
- ACL reconstructions in children has more than tripled over the last 15 years
How does the risk of an ACL injury differ between males and females?
- Female athletes are 2-10 times more likely to injure their ACL than males playing the same sport
- In football, females are 3-5 times more likely to injure their ACL than males
- In basketball females are 2-7 times more likely to injure their ACL
- For non-contact injuries in football, females are more likely to injure the ACL of their supporting leg and males tend to injure their kicking leg
Why women have higher risk of ACL Injury?
- Anatomical Differences:
- Higher BMI (Body Mass Index – a measure of obesity)
- Wider pelvis puts greater valgus stress on the knee
- Increased hypermobility and joint laxity
- Smaller notch (part of the knee where the ACL sits) puts ACL at risk of impingement
- Biomechanical:
- Poorer landing technique (commonly the knees come together when landing putting additional valgus stress on the knee)
- Reduced knee and hip flexion during landing puts greater stress on the ACL
- Fatigue resistance: some research suggests increased propensity in females to fatigue (tire out) earlier and this increases risk of ACL injury
- Neuromuscular:
- More quadriceps dominant than males (weaker hamstrings to quadriceps power ratio)
- Weaker core stability
- Have 4-6 higher risk of ACL injury than men participating in same landing and pivoting sports
- Hormonal (Effect of menstrual cycle):
- 2.4 times greater risk of ACL injury in pre-ovulatory (first half of menstrual cycle) than post-ovulatory phase (second half of menstrual cycle)
- Hormonal effect on increasing laxity (and therefore risk of ACL injury) is highest during ovulation
- Highest risk of ACL injury thought to be a week before and shortly after period
- Oestrogen receptors have been found on ACL ligaments
- Some research has shown oral contraceptive pill may reduce risk of ACL
- Landing biomechanics change during ovulation putting the ACL at risk:
- Knee collapses more into valgus (midline)
- Hip internally rotates more on landing
- Genetic:
- A major structural component of ligaments and tendons is a protein called collagen: specifically type I and V collagen
- A gene that encodes for the alpha1 chain of type I collagen (COL1A1) has been shown to be associated with increased risk of cruciate ligament rupture
- A gene that encodes for the alpha1 chain of type V collagen (COL5A1) has been shown to be associated with increased risk of Achilles tendon injury
- The CC genotype of the COL5A1 gene has been found to be underrepresented in females with ACL injuries
What are the symptoms following an ACL tear?
- Very painful with patient often writhing around in agony
- Often hear and feel a pop inside the knee
- Very swollen knee that comes on rapidly
- Typically unable to carry on playing during a game and if they do, they feel the knee give way when they change direction
- If there is a displaced meniscal tear the knee can lock (inability to straighten out the knee) and need prompt medical assessment if suspect this
- If a patient tries to play sport following an ACL tear and once the knee swelling subsides, they will have a feeling of instability with the knee buckling under them and they will be unable to reliably:
- Jump and land on the knee
- Accelerate and decelerate
- Rapidly change directions
- Rapidly pivot on the knee
What should you do if you suspect you injured your ACL?
- Be escorted with assistance from field of play
- Rest, ice and elevation – will help to reduce swelling which is key to relieving pain and regaining range of motion to the knee
- Use crutches and try not to weight bear
- Seek medical help soon as possible
How is an ACL tear diagnosed?
- History of the injury can be very suggestive
- Examination of knee can detect ACL tear in more than 80% cases
- MRI scan: over 95% detection rate but not quite 100%
- MRI scan can detect additional injuries:
- Meniscal tear: occur in 50-75%
- Collateral ligament injury (most commonly medial): ~45%
- Partial tears of the ACL ligament are recognised but difficult to tell accurately what percentage is intact from the MRI scan:
- Decision for treatment depends on clinical and examination findings of instability
- Patient’s physical demands and expectations
- Partial ACL tear can be augmented rather than fully replaced
- During arthroscopy: the definitive confirmation for ACL injury
Does every ACL injury need an operation?
- In short no
- Conservative management would be suitable for:
- Older patients
- Less physically demanding patients
- Presence of moderate to severe knee osteoarthritis
- Those who do not have feeling of instability during everyday activities
- Those who are happy to restrict their activities to exercises that put less rotational stresses to the knee such as straight-line jogging on level ground, cycling, and rowing
- ACL reconstruction can be carried out at a later date if appropriate:
- Patient should have had a good course of physiotherapy, and despite this is still having episodes of instability or
- Patient wishes to go back to more competitive and rotationally demanding sports
- Rehabilitation can be more painful due to lack of protection of an intact ACL
- Higher risk of meniscal injury when the knee gives way which then increases the risk of developing osteoarthritis:
- The incidence of meniscal tear (especially medial) in the presence of chronic ACL instability is 75-90%
When would surgery for ACL injury be suitable and how is it carried out?
- Details on ACL reconstruction can be found here
More relevant information can be found on:
- ACL Injury Prevention Programme
- ACL reconstruction
- The benefits of adding Lateral Extraarticular Tenodesis to an ACL Reconstruction
- ACL Graft Options